
Non-Sinus
P wave morphology is not consistent with sinus (including inverted P in lead I)
|
Normal Rate:
|
Fast Rate:
|
Ectopic Atrial Rhythm
- P waves are abnormal in both limb leads and chest leads
CLINICAL SIGNIFICANCE
- Not much
- No treatment is necessary
- Rarely associated with atrial tachycardia
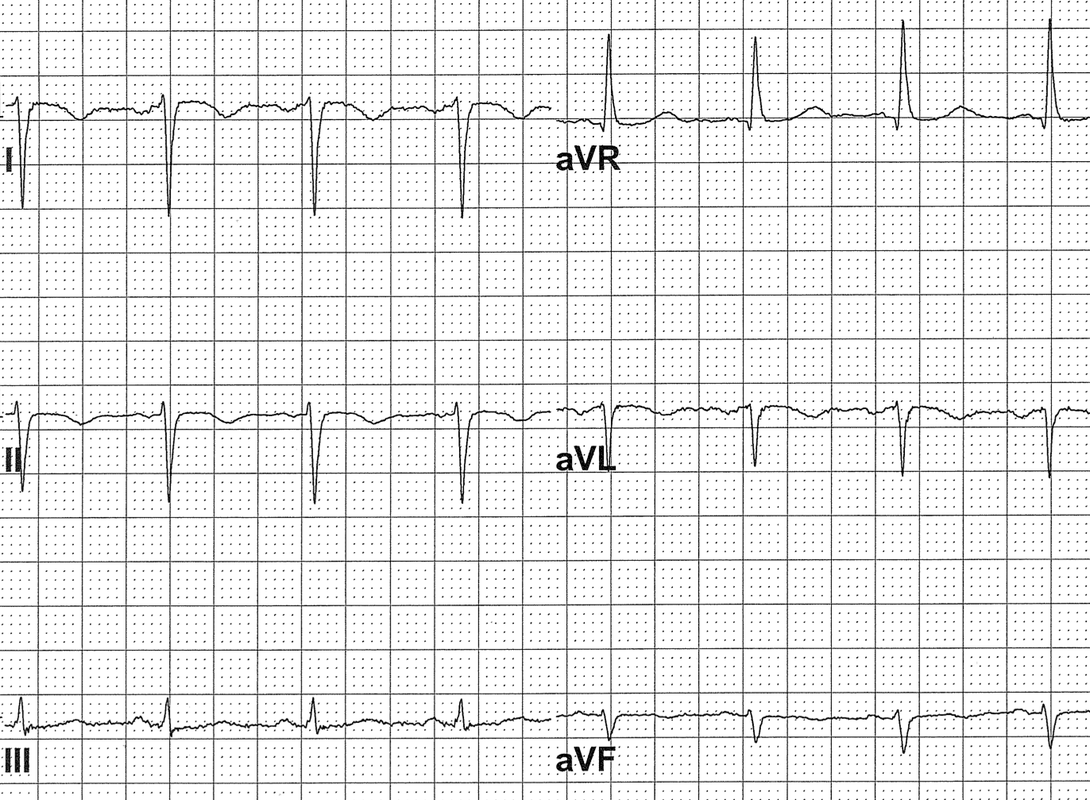
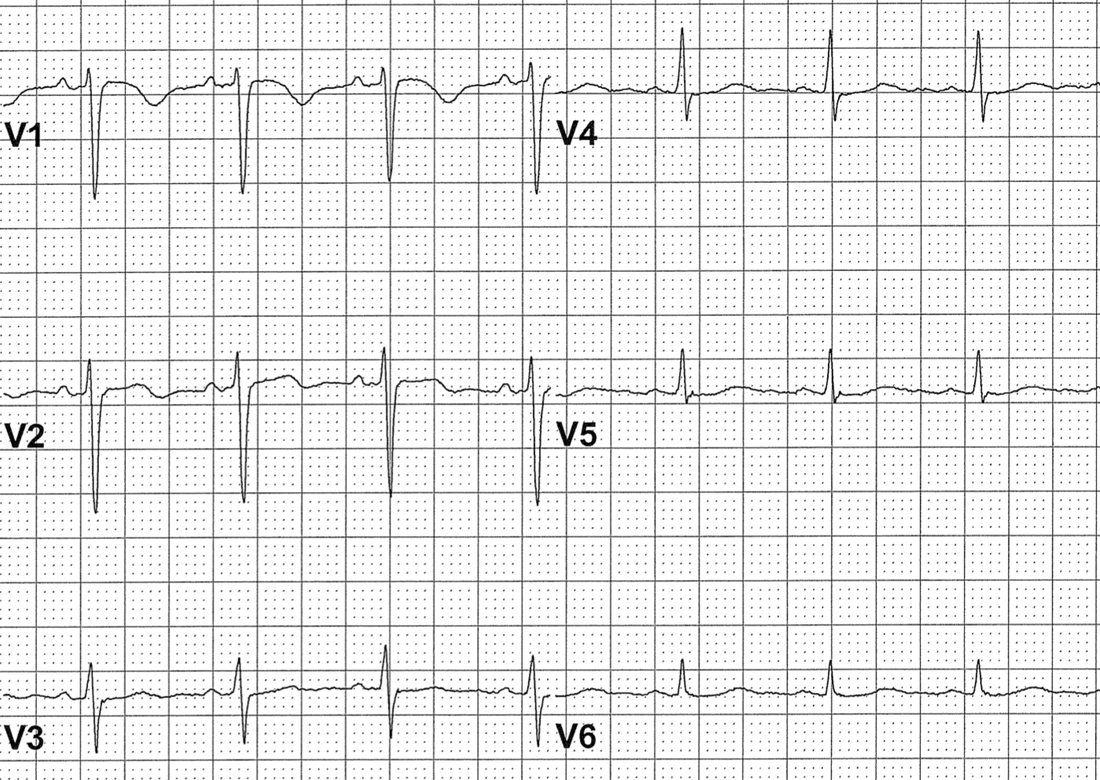
DEXTROCARDIA
- Both P and QRS are inverted in lead I
- QRS progression is reversed in chest leads
CLINICAL SIGNIFICANCE
- ECG is not interpretable and may mimic MIs, fascicular blocks, ischemia
- Repeat ECG with everything reversed
LIMB LEAD REVERSAL
- P waves are normal in the chest leads
- QRS may be inverted in lead I
- Lead II may look like a flat line
|
|
CLINICAL SIGNIFICANCE
- Must repeat the ECG!
- Limb leads are bipolar leads
- Limb lead reversal may mimic and mask MIs, fascicular blocks, low voltage, hypertrophy, ischemia
- Lead reversals are very common
Retrograde P waves
- P waves follow the QRS complexes
- P waves have “retrograde morphology”
- negative in II, III, aVF
- usually upright in V1
- Following junctional QRS complexes
- junctional rhythm or junctional tachycardia
- Following ventricular QRS complexes
- idioventricular rhythm or VT
- Following ventricular paced complexes
CLINICAL SIGNIFICANCE
- When you see an obvious narrow-QRS tachycardia but the computer “thinks” it is a wide-complex tachycardia:
- It is almost always reentrant PSVT where the retrograde P waves are measured as if they were part of the QRS complexes
- Pacemaker Syndrome
- Chest discomfort, shortness of breath related to abnormal pacemaker syndrome
- Most common in ventricular pacing with 1:1 retrograde conduction
- Neck veins: “cannon JVPs”
- Left atrium: “cannon PVPs” (cannot see)
- Either due to ventricular pacer or A-V pacemaker with atrial lead malfunction
- Treatment: upgrade the pacemaker
- Chest discomfort, shortness of breath related to abnormal pacemaker syndrome
Artifact
- Parkinsonian tremor
- High frequency oscillatory ventilation
- Both are typically 5 Hz artifacts
- 5 Hz = 300/min which is the usual atrial rate in atrial flutter
- Clues for distinguishing artifact from flutter:
- Flutter waves are typically sharp
- Flutter waves are typically negative in II, III, aVF
- Sinus P waves are present
CLINICAL SIGNIFICANCE
- Parkinsonian tremor and HFOV are frequently mistaken for Atrial Flutter
- Inappropriate treatments including electric cardioversion have been described
Ectopic Atrial Tachycardia
- Atrial rate 110-220
- P wave morphology is abnormal in the limb leads and the chest leads
CLINICAL SIGNIFICANCE
- Usually a marker of “sickness”
- Usually does not require treatment
- difficult to suppress
- ventricular rate equals atrial rate
- Anticoagulation is usually not indicated
Atrial Flutter
- Atrial rate 230-380
- Extremely common arrhythmia in sick hospitalized patients
- Flutter waves are typically sharp and negative in leads II, III and aVF
- Flutter waves are typically upright in V1
- Atrial Flutter with 2:1 conduction is the most common regular SVT outside of sinus tachycardia in hospitalized patients
atrial flutter red flagsFrequently missed by the interpretation software and by physicians Think about atrial flutter if the computer read out says;
|

|
Multiple P Wave MOrphologies with Variable PR Intervals
- Rate <100: wandering atrial pacemaker
- Rate >100: multifocal atrial tachycardia
- Frequently read as atrial fibrillation
- Frequently associated with decompensated lung disease, critical illness, postoperative state
- No anticoagulation, no digoxin, no cardioversion
- May treat with diltiazem or beta blocker if symptomatic