
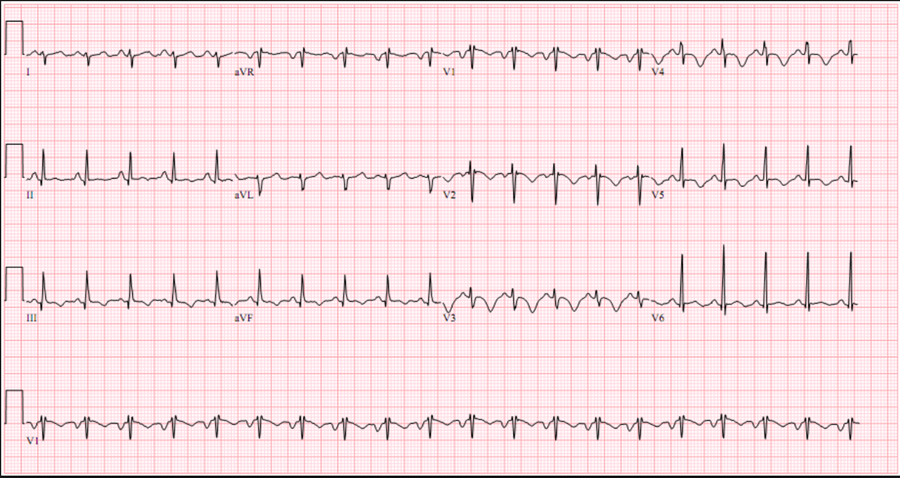
Pulmonary Embolism
- The sensitivity of the ECG to diagnose PE is very low
- The specificity of ECG signs suggestive of PE is very low
- The ECG signs are only useful if they are not known to be old
- The ECG may direct you to consider PE under the appropriate clinical scenario
- The most important unfavorable prognostic sign is new incomplete or complete RBBB
- Sinus tachycardia: important “company” for all other markers
- SI – QIII - TIII pattern: S wave in lead I >1.5 mm; Q wave and inverted T in lead III
- Incomplete or complete RBBB: rSR’ in V1
- T wave inversion in V1-V3: mimics anterior ischemia
Clinical SigNificance
- It signifies hemodynamic severity
- Poor prognosis, high mortality
- May want to obtain stat echo
- Consider lytics
- Consider pressors
- Use caution with vasodilators
- Be careful with intubation