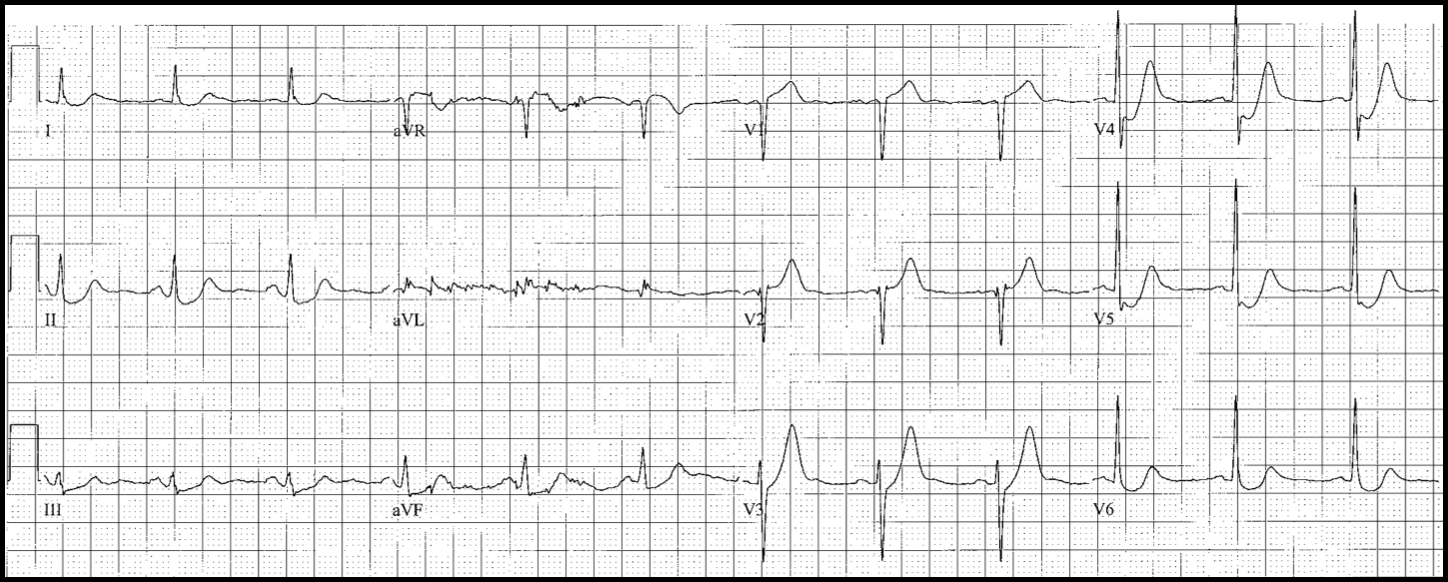
STEMI
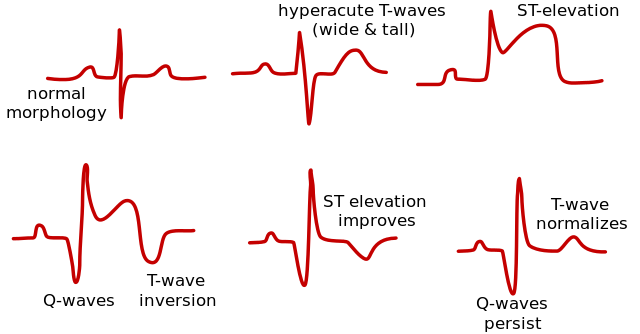
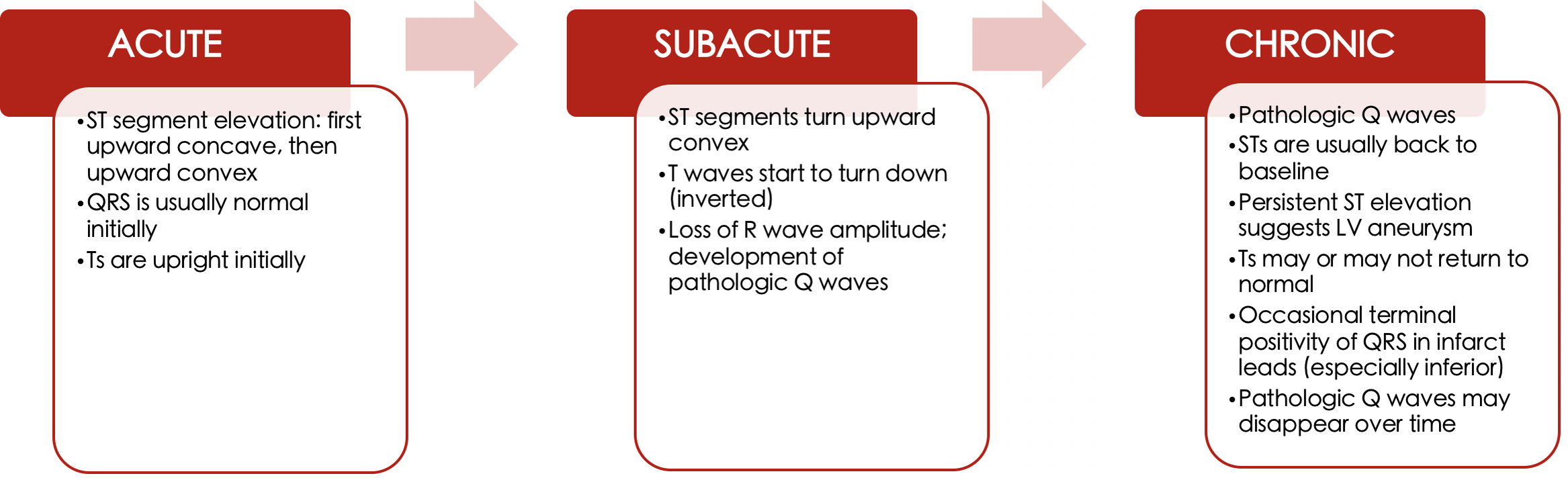
Time course of ECG progression
- Variable; phases may be skipped
- ECG progression is modified by reperfusion therapy
ECG Leads |
Location of MI |
Probable Culprit |
II, III, aVF (±V5,V6) |
Inferior |
RCA (or dominant LCX) |
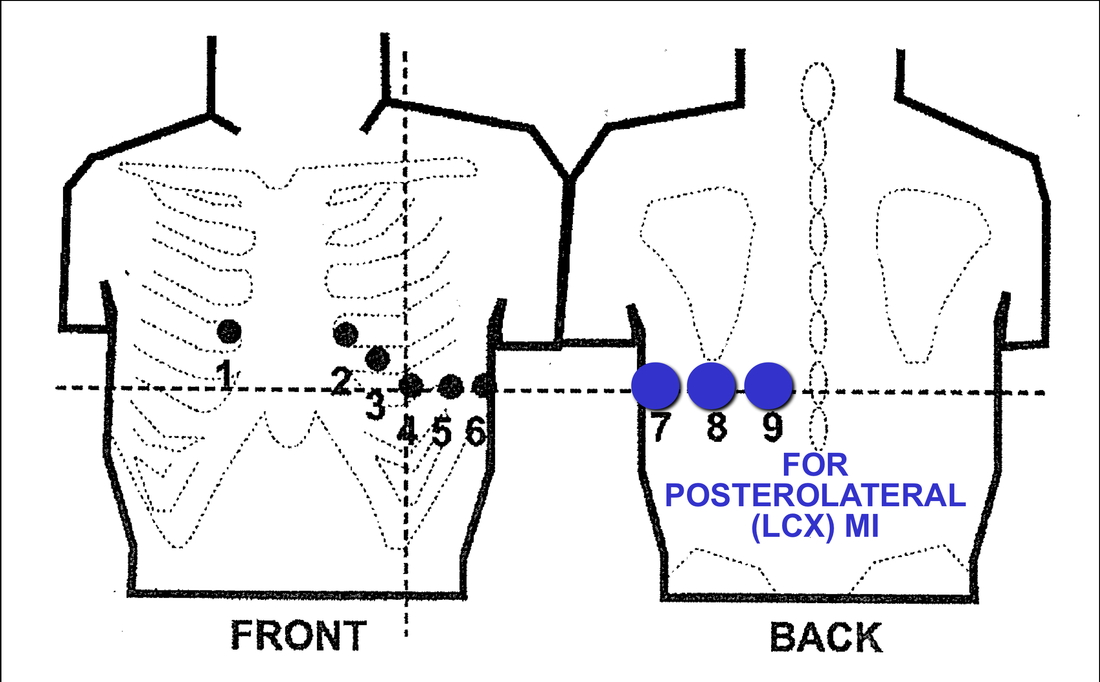
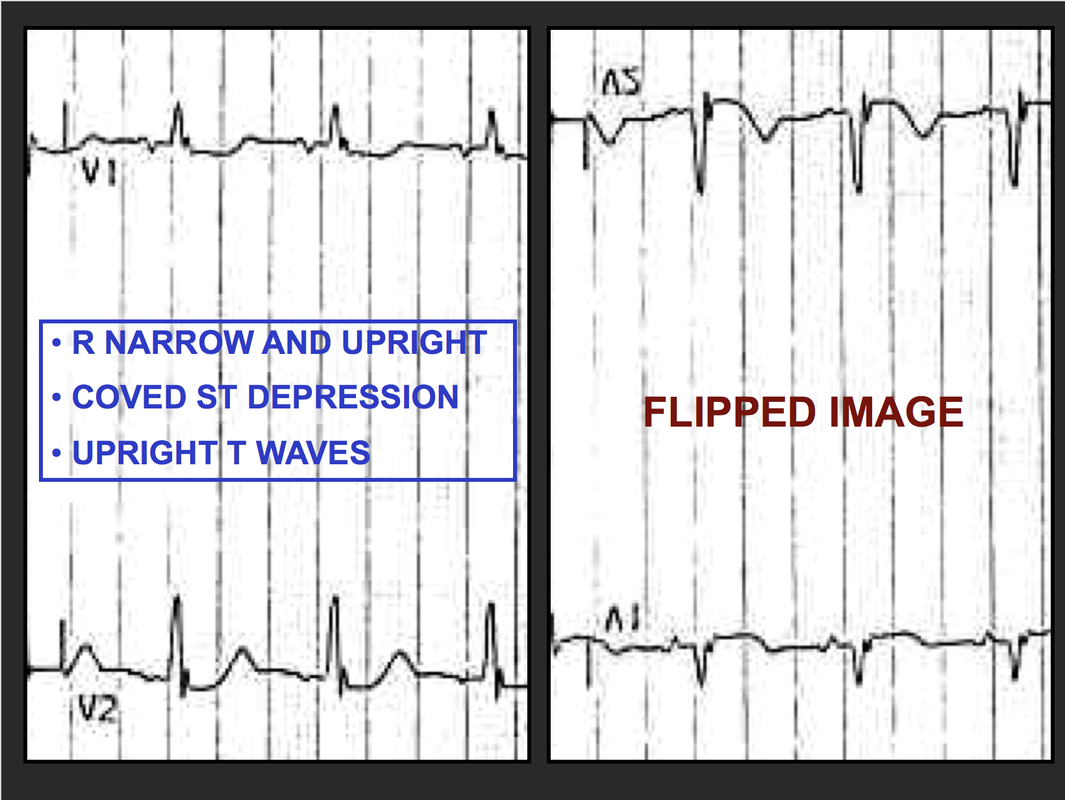
Mirror image V1-V2 (R, ST¯, T) |
Posterolateral |
LCX |
II-III-aVF, plus V1 and RV4 |
Inferior + RV |
Proximal RCA |
V1-V4 |
Anteroseptal |
LAD |
V1-V6 (± I, aVL) |
Extensive Anterior |
LAD |
I, aVL, V4-V6 |
Lateral |
LCX |
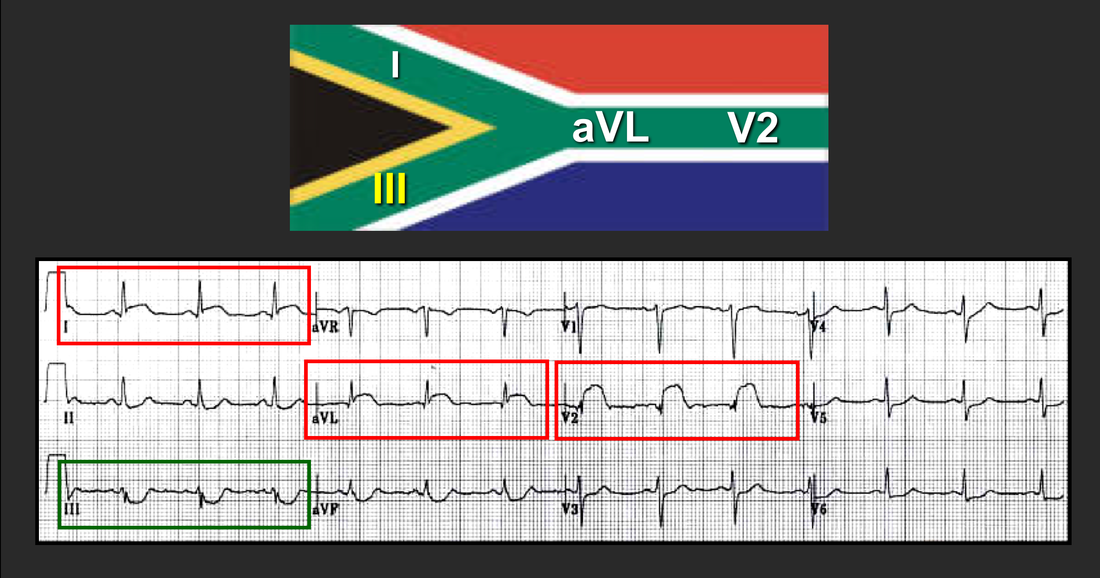
I, aVL, V2 (± mirror image III) |
High Lateral |
LAD-D1 |
|
FREQUENTLY MISSED MIs
Posterolateral (LCX)
|
|
|
|
ST Depression in V1-V4, subtle ST Elevation in I, aVL
|
High lateral
|
|
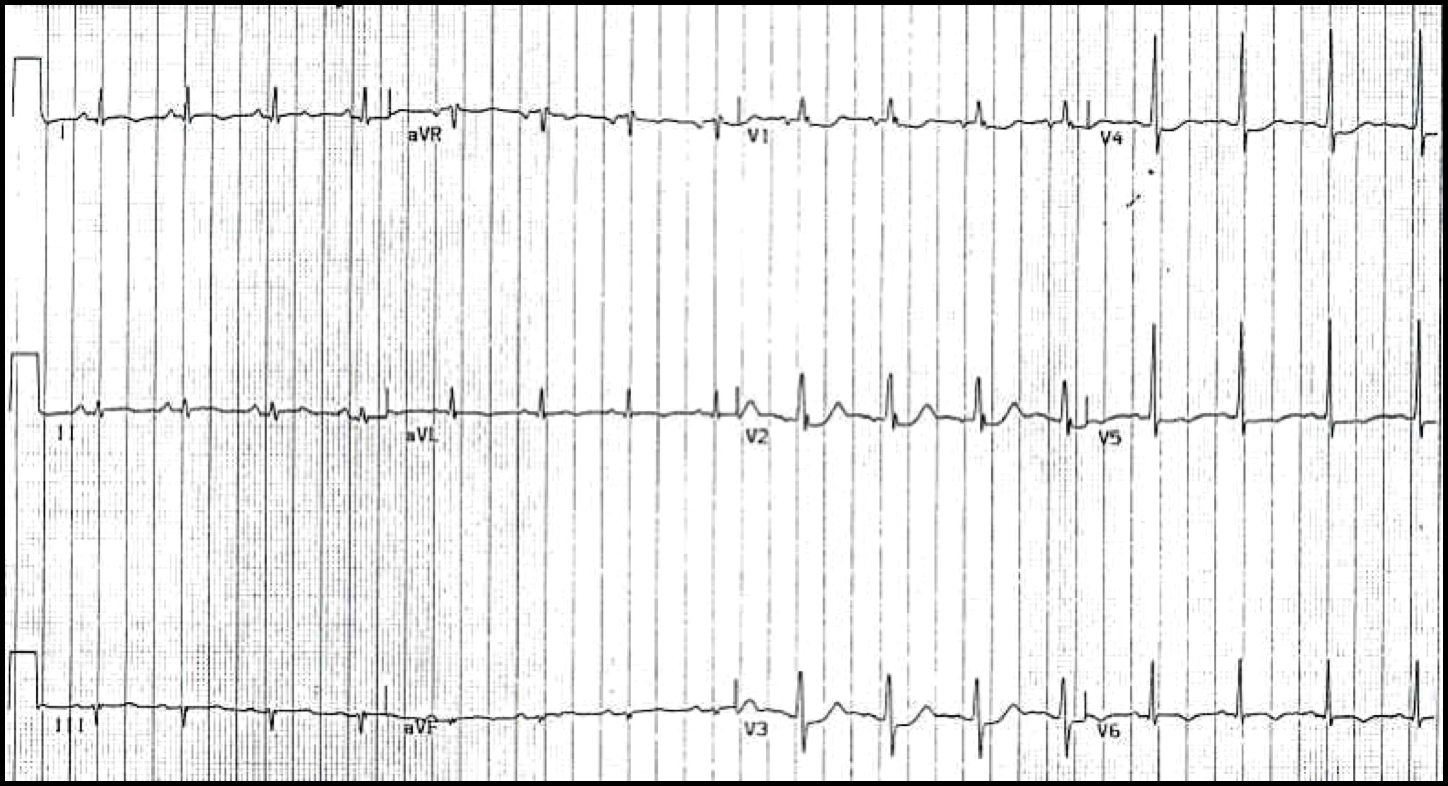
RV infarct
- Almost always in association with inferior MI
- ST in R-sided chest leads; sometimes in V1; rarely in V1-V4 (may mimic anterior STEMI)
- Combination of ST in inferior leads plus ST in V1 is highly specific for RV infarct
- Frequently associated with sinus bradycardia or atrial fibrillation with AV block
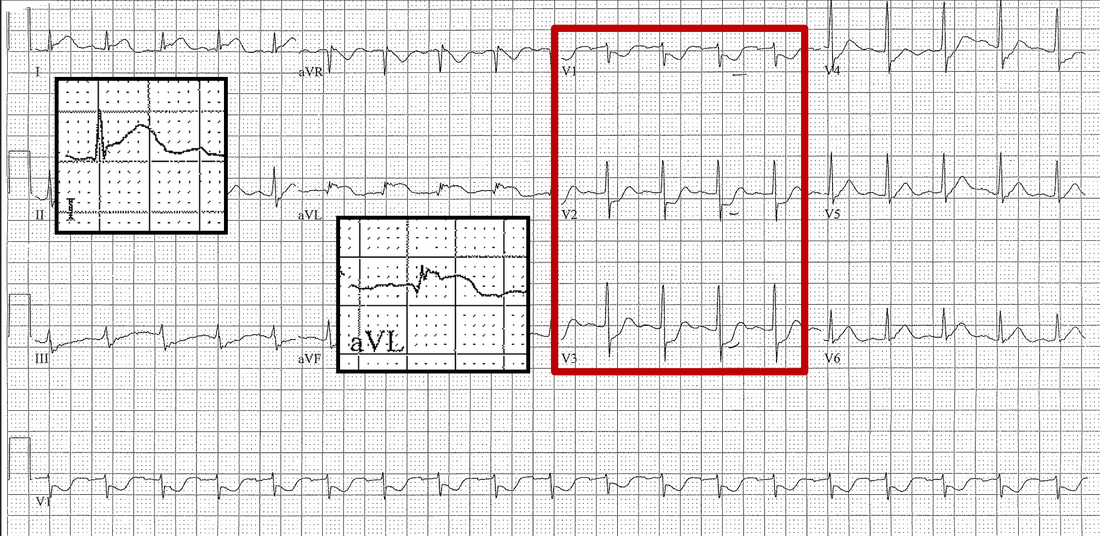
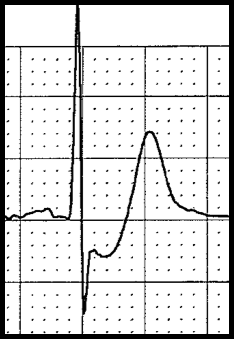
Anterior “STEMI” without ST elevation
- J-point depression followed by upsloping STs in the anterior chest leads
- Very tall (“hyperacute”) T waves usually taller than the corresponding QRS complexes
|
DeWinter's Sign
|
|